Becker's Healthcare Webinar
Poster
CNS 2025 — Poster #46
Speed and Accuracy of an AI-Automated Medical Record Screening Tool for Therapeutic Clinical Trials




98.1%
PDF Record Accuracy
99.7%
HIE Record Accuracy
2.6 min
Median Processing Time (PDF)
Abstract
Background
The recruitment of medically qualified patients is a major bottleneck in therapeutic clinical trials. Traditional manual screening methods are cost and labor-intensive, requiring up to 8.8 hours per enrolled patient per study.
Objective
To assess the speed and accuracy of an AI-automated medical record screening tool for therapeutic clinical trials.
Design
Retrospective chart review.
Results
We observed an overall question accuracy of 98.1%, a false negative rate of 0.46%, a false positive rate of 7.41%, and a median processing time of 2.60 minutes for PDF records. For Health Information Exchange records, we observed an overall question accuracy of 99.7%, a false negative rate of 0.24%, a false positive rate of 0.77%, and a median processing time of 4.31 minutes.
Conclusion
Our platform demonstrates the potential to drastically reduce the time and cost associated with manual medical record review for screening and medical qualification of patients into therapeutic clinical trials.
Methods
We retrospectively reviewed data on medical records of patients which were retrieved and analyzed between August 1, 2025 to September 30, 2025 as part of the recruitment efforts across 61 distinct therapeutic protocols. Medical records on patients were obtained through an AI-assisted process which integrates with multiple data sources including Health Information Exchanges (HIEs), pharmacies, imaging networks, EHRs, and other sources. Records unavailable through digital networks were retrieved via direct outreach to providers.
I/E criteria for each trial were manually extracted from the clinical trial protocol provided by the sponsor or site. The I/E criteria for each protocol were then transformed into a set of machine learning prompts or questions designed to be answered from the medical records with a binary yes/no response.
Retrieved medical records consisted of 2 different record types: (1) unstructured PDFs and (2) semi-structured data retrieved from Health Information Exchanges (HIEs).
Overall, we analyzed 1,569 PDF records against one of 54 unique sets of I/E criteria consisting of between 10 and 206 yes/no questions each. Overall we assessed 400 distinct yes/no questions, each of which had at least 50 observations for a total of 68,035 question-answer pairs.
Similarly, we analyzed 1,118 HIE records against 7 unique sets of I/E criteria, consisting of between 10 and 206 yes/no questions each. Overall we assessed 192 distinct yes/no questions, each of which had at least 50 observations for a total of 76,957 question-answer pairs.
Each question-answer pair included in this analysis included citations to page sources within the medical record, and was reviewed for accuracy by a trained human clinical reviewer.
Processing Time Estimation
Processing time was estimated on a sub-sample of 200 HIE records and 705 PDF records by comparing timestamps in processing records. We also evaluated the size (number of rows) for each of the 200 HIE records to determine the relationship between document size and processing time.
Aug 1 – Sep 30, 2025
Date Range
61
Protocols
1,569
PDF Records
1,118
HIE Records
68,035
PDF Q-A Pairs
76,957
HIE Q-A Pairs
Results
We observed an overall question accuracy of 98.1% for PDF records and 99.7% for HIE records (Figure 1).
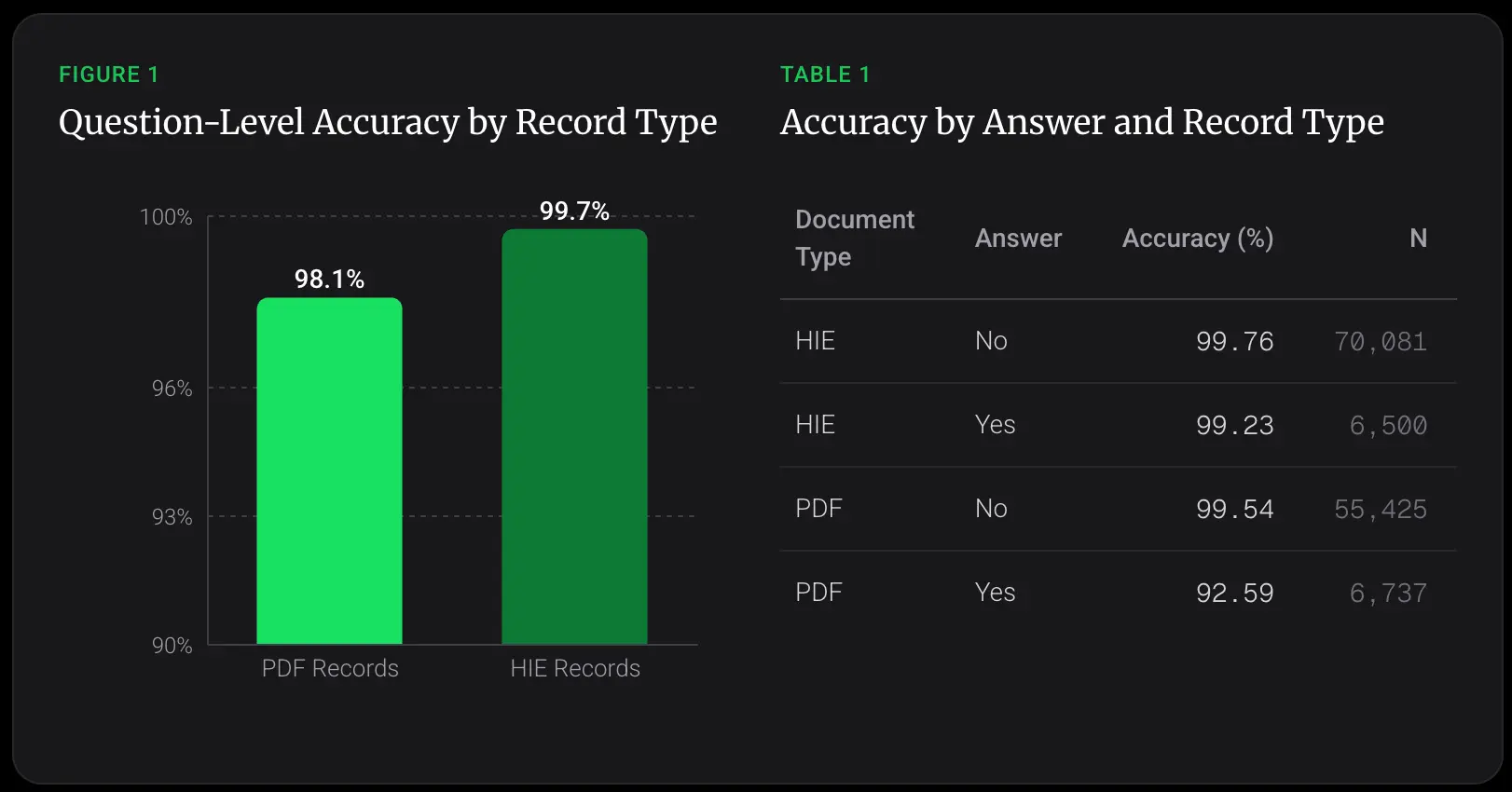
We also evaluated accuracy according to whether the answer to the clinical I/E criteria question was determined to be a "yes" or "no" by the machine learning tool, as measured against the final determination by a trained human clinical reviewer.
For HIE records, we observed a false negative rate of 0.24% and a false positive rate of 0.77%. For PDF records, we observed a false negative rate of 0.46%, and a false positive rate of 7.41% (Table 1).
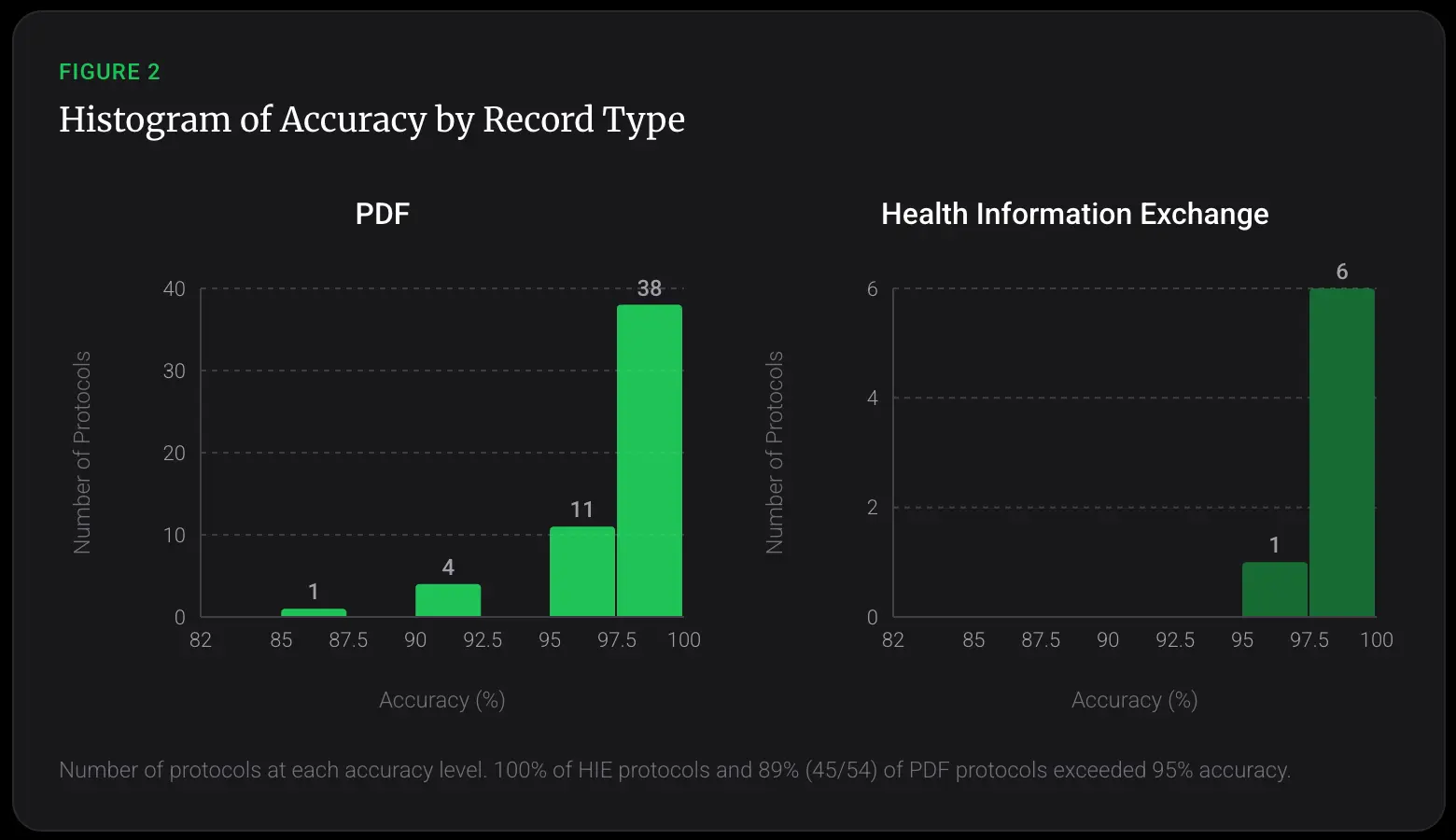
We analyzed accuracy across protocols (sets of I/E criteria consisting of multiple yes/no questions). For HIE records, 100% of protocols were answered with greater than 95% accuracy. For PDF records, 89% (45/54) were answered with greater than 95% accuracy (Figure 2).
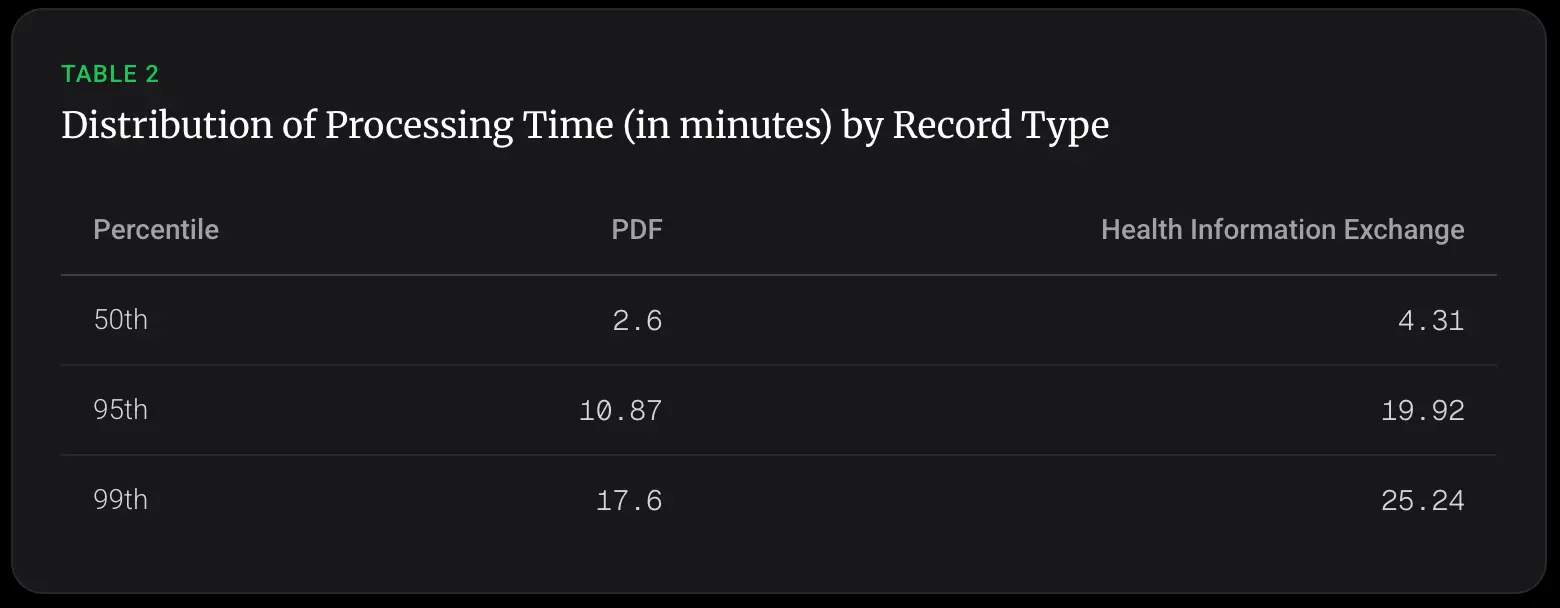
We also measured the distribution of processing times for different document types. For PDF records, we saw a median processing time of 2.60 minutes, with a 99th percentile of 17.6 minutes. For HIE records, we saw a median processing time of 4.31 minutes with a 99th percentile of 25.24 minutes (Table 2).
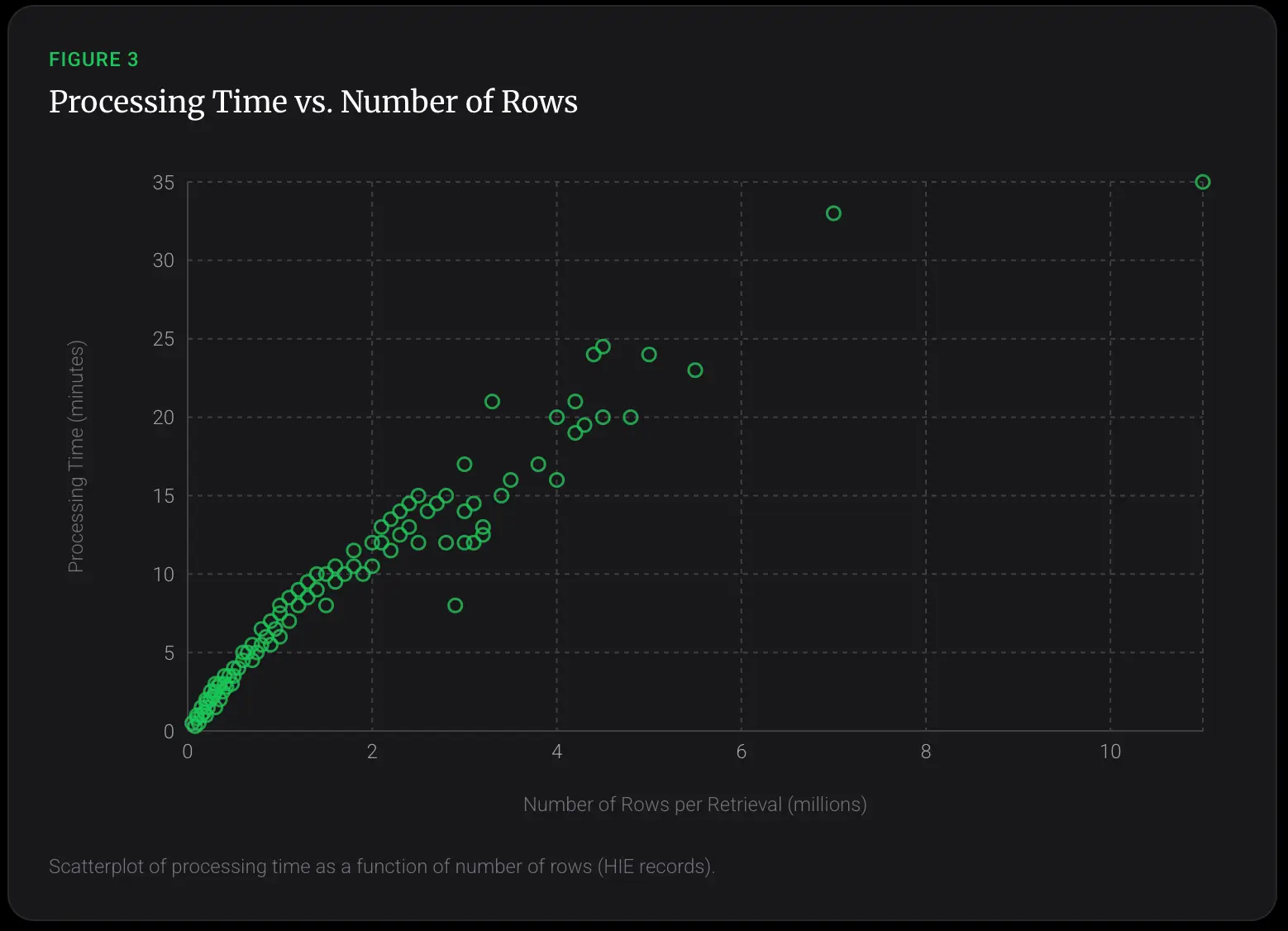
By analyzing HIE records, we found that processing time increased with document size. Processing time was correlated with the number of rows in the HIE record, suggesting that larger records take longer to process.
Discussion
Our platform achieved 98.1% accuracy on unstructured PDF records and 99.7% on semi-structured HIE records, with median processing times of 2.6 and 4.3 minutes respectively -- vastly outpacing the multi-hour manual benchmarks that currently strain sites and coordinators, while preserving and likely exceeding the clinical accuracy of human clinicians.
The exceptionally low false-negative rates (0.24-0.46%) observed here are reassuring in that they minimize enrollment oversights.
We did observe an unusually high false positive rate (7.41%) across PDF records. These are instances where the machine learning tool answered "yes" to a clinical trial eligibility screening question, but that a trained human clinical reviewer later determined, upon manual review of the medical record, should have been answered as a "no".
This high false positive rate is likely a result of the unstructured and varied nature of PDF based medical records. Given that this tool provides citations to page sources within the record, and is used by coordinators as a tool to amplify and accelerate, but not replace the final clinical judgement of the coordinator or investigator, we do not expect this false positive rate on PDF records to result in incorrect randomization into a clinical trial.
We observed > 95% accuracy of the tool across 89-100% of questions and protocols, which demonstrates dependable performance across varied clinical protocols.
Limitations include medical records and data which were limited to that which was obtainable from previous providers and the HIEs, a limited and varied number of therapeutic areas and sites, lack of visibility into the final determination on enrollment for each patient, and a limited sample size and time window. Future efforts will require evaluation across an increased number of records, sites, clinical trials, and disease states.
These results demonstrate the potential of artificial intelligence to efficiently perform clinical trial screening in minutes instead of hours, and greatly reduce the cost and increase the velocity of clinical trial enrollment.
References
1. Unlu O, et al. Manual vs AI-Assisted Prescreening for Trial Eligibility Using Large Language Models -- A Randomized Clinical Trial. JAMA 2025;333:1084-1087.
2. Penberthy LT, et al. Effort Required in Eligibility Screening for Clinical Trials. J Onc Pract 2012;8:365-370.
Disclosures
The authors are compensated employees of Predoc.
Download the Full Poster
Get the complete research poster as presented at CNS 2025.
Get Complete, Usable Patient Data.
Stop manually chasing and cleaning records. See how Predoc seamlessly integrates with your existing systems to deliver normalized, actionable data right when you need it.


